Sitaram Bhartia Institute of Science & Research
B-16, Qutab Institutional Area, New Delhi, 110016
+91-9811109833, 9810446857
Partial Knee Replacement (Capping) (Video Link - Partial Knee Replacement)
It seems that you have tried all measures to control your knee pain, and it is becoming obvious that some sort of surgery will be required to fix your problem. The surgery at various stages of arthritis is different. The following are the operations commonly performed for knee arthritis.
- Key-hole surgery (Arthroscopic Surgery)
- Alignment correction (High tibial osteotomy or HTO)
- Partial knee replacement (Unicondylar Replacement or Capping)
- Total knee replacement (Knee Arthroplasty or TKR)
After doing necessary tests, your doctor has suggested to you that 'capping' or what is commonly called 'partial knee replacement' is the best option for you. Though, it is a wellestablished operation with over 30 yrs. of experience abroad, it is relatively new in India. In this brochure, we would like to educate you about this operation.
Know your knee joint
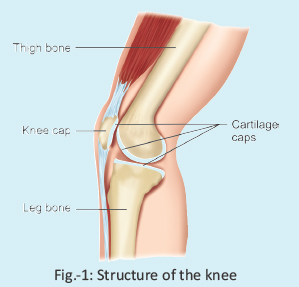
The knee is made up of three bones – the thigh bone (femur), the leg bone (tibia), and the knee cap (patella). All these bones are covered with smooth-like-butter, soft cap, called cartilage (Fig-1). When a joint moves, it is the cartilage caps which makes it frictionless. With age or due to injury these caps wear out, and the bone-ends become raw. This is called arthritis, though it is known that changes of arthritis may not affect the whole joint.

From an understanding viewpoint, it may be considered that the knee is made up of three parts (compartments) - one on the inside (medial), one on outside (lateral), and one in front - the knee cap joint (Fig-2). The arthritis may affect one, two or all the three compartments of the joints. If only one compartment is affected, it is termed unicompartment osteoarthritis. Treatment is different if it is unicompartment osteoarthritis than when all the three compartments are affected.
What actually is partial knee replacement?

Now-a-days, when only one compartment of the knee is affected, it is good enough to replace only that part. This is called capping or partial knee replacement (Fig-3). This is a new concept, unlike what used to be done in the past, when the only treatment of a damaged knee, whether fully or partially damaged, was to do full knee replacement. Putting a cap on the damaged part of the knee is something similar to what a dentist does, when he puts a cap on top of a broken tooth rather than replacing it. In rightly chosen patients, it works nearly as well as a knee replacement. The only caveat is that the damage must be limited to only one compartment. Capping or partial replacement can be done only in a 'window period'- not too early, not too late.
Once we are operating, why not replace the whole knee?
This is a natural thought that comes to one’s mind. Also, surgeons who do not practice partial knee replacement, often give this argument. But if one thinks of it, why replace full when you can do with partial. God-given knee is always better than man-made, and should be preserved as long as possible. Fully replaced knee is never as good - there are limitations which one has to observe. Hence the trend is that if arthritis affects a younger person, one should try to preserve the original knee as long as possible with less invasive operations (joint preservation operations). It is therefore logical to do only partial replacement, wherever suitable.
Am I not too young for a knee operation?
There is no age for an operation. It is done if the person is suffering from knee pain, and the pain is not resolved by non operative means-whatever the age may be. Partial knee replacement is a knee preservation operation as nothing is removed from the knee. This is meant for extending the life of the original knee. It is done for younger people whose knee is damaged only partially.
How do we know that the joint is only partially damaged, and is suitable for capping?

There are a number of ways doctors can make out whether only a part or whole of the knee is damaged. Clinical examination and some special X-rays give a fair idea. For example, if your pain is limited to inside of your knee, you may be a candidate for partial knee replacement (Fig-4). In doubtful cases, one can perform arthroscopy (look inside the knee with a camera) just before the actual operation.
How do you compare partial (UKR) and full (TKR) ?
| Issues | U.K.R | T.K.R |
|---|---|---|
| When? | Only partial damage | More damage |
| Cut | Smaller (50%). | Larger |
| Ligament | Left untouched | 2/4 removed |
| Bone removal | Only a slice removed | Ends reshaped |
| Walking | 2 days with stick | 3 weeks with stick |
| Independent | 3 weeks | 8 weeks |
| Feel | Like a normal knee | Like a foreign part |
| Back up option | Full replacement | Repeat full replacement |
What will happen if I delay the operation?
There is a window in which partial replacement can help - not too early & not too late. A lot of patients in early stage of arthritis may not feel disabled, and may not like to go for full replacement. Such patients usually decide to live with the pain. In such early cases, when the arthritis is limited to one compartment, the balance of the knee is regained by capping (partial replacement), and the progress of the arthritis is thus halted. If not done, the arthritis progresses to other compartments, eventually landing one into knee replacement.
How successful is the operation?
This is one of the good knee operations. Pain relief is nearly complete. The shape of the legs improve as also the gait. Nearly 90% patients feel well upto 15 yrs. Appropriate patient selection and proper surgical technique is the key to success of the operation.
Unlike knee replacement, partial replacement gives the feel of a normal knee as all the ligaments are untouched. One gets full bending of the knee and there are no restrictions on siting on the floor, siting cross-legged etc.
Is the operation painful?

The thought of operation brings the thought of pain. Though every operation is associated with some pain and discomfort, partial replacement is a smaller and hence relatively less painful operation. With the use of modern pain control techniques, it has been possible to make this operation nearly pain-free (Fig.-5). Our team is particularly sensitized to ensure a pain-free surgery, and do everything to make your operation so.
What is the life of replaced partial knees?
The capping lasts for 15 years in upto 95 percent of cases, but can last even longer. The ones failing, can be fixed again by going in for replacing the whole knee. This makes it a better option than straight away going for knee replacement, because if knee replacement fails due to any reason, replacing full to another full is a relatively major operation.
How long does it take to recover?

You will be in the hospital for 3 days. You will be admitted one day prior to surgery for fine tuning of your medical condition and will be operated the next morning. The operation takes on an average, one hour for one knee. You will be in post–op recovery area till the evening of the operation, and then shifted to your room. Gentle physiotherapy is started from the day after surgery. A typical recovery schedule for those who get one knee capped as shown below.
Can both the knees be operated at the same time?
Yes, it is very much possible and is our routine practice for the last 10 years. There is enough evidence to support that in selected cases, the success rate of doing both knees together is no different from doing them one by one.
How much does this operation cost?
Cost may vary depending upon the technique and the implant used. You may discuss this with your doctor when you come for scheduling the surgery. We have packages for different categories of patients. As a ball mark figure it costs 1.5 to 3 lacs* for each knee.
Which implant do we use?

We use best quality imported implants which have a long track record. The one we use is called 'Oxford Uni'. It is a mobile bearing knee, which means that there is a 'free moving' plastic piece between the two steel caps fixed on the two bones (Fig-6).This gives longer life to the knee as the plastic does not wear out so easily. There are a lot of new implants coming in the market all the time. We keep ourselves updated with all the new developments and carefully choose the one best for our patients.
What is the procedure of getting operated?
Once you decide to get operated, our team will take over. They will explain you the whole procedure, which consists of finalizing the date for surgery, and backward planning thereon. You will need to do the following:
- General health check to assess whether you have any health issues which need attention. This will involve a visit to the anaesthetist who will certify your fitness for surgery.
- Physiotherapy
- Dietary advice
- Health insurance related or payment related issues.
A thorough check up is done before surgery to make sure there is no obvious risk involved in surgery. The operation is usually not done under general anaesthesia, but under spinal anaesthesia (injection in the back, which makes the legs numb). You will be awake all through the operation, but will have no feeling in the legs. You will not come to know anything as you will be put to sleep by medicines. Most patients have a pleasant experience of the operation, and say that they “did not come to know when the operation started and finished”.
What is the post-operative requirement?
Once you are discharged from the hospital, approximately 3 days after the surgery, our home care team will take over under guidance of our chief physiotherapist. This is done considering the difficulty faced by patients in visiting the hospital repeatedly. They will organize physiotherapy as well as stitch removal at home. You always have the choice of coming to the hospital to get the stitches removed.
What complications can occur?
Capping is a fairly complication free operation, but like in any operation, complication can rarely occur. We keep our complications to minimum possible by taking all precautions and following international norms. In a rare case, if a complication does occur, we take immediate corrective measures. With this aggressive approach, we have been able to keep our complication rate low. The following is an account of some of the more common complications - just to inform you, and not to alarm you. This is by no means a complete account, though the commoner ones you should know.
Anaesthesia related complications: Nausea, vomiting, giddiness, headache are not uncommon complications of surgery, but can be promptly controlled by medication. Very rarely, allergic reactions to medication can occur.
Swelling and blood accumulation in the knee: This surgery is performed under tourniquet control, which means during surgery, the blood supply to the limb is completely stopped by using a pressure band on the thigh (tourniquet). Once the same is released at the end of the operation, some blood oozing may occur and collect inside the knee. If required, such collected blood is removed with a needle and syringe, under local anaesthesia.
Wound healing issues: Redness around the wound and some watery discharge is not uncommon. Heals with time and care.
Infection: Infection is a dastardly complication of any surgery, and may happen in one in 300 cases. We take all precautions and check that you are not carrying any infection in your body which may travel to the operated area.
Deformity and stiffness of the knee: Some knees are prone for getting stiff, either by themselves or due to lack of proper post op rehab. They need concerted effort by the patient and the physio, and usually recover.
Loosening: Sometimes the artificial caps, which are fixed to the native bone with the help of bone cement, get loosened. The reason may be: not a perfect fitting implant, poor bone quality or injury. Fortunately this happens only in 1/100 cases, and may have to be rectified by repeat surgery.
Our technique of partial knee replacement (Capping)
Partial knee replacement is not as common an operation as knee replacement. We are the pioneers in this surgery in north India. This is so because we are knee specialists and not merely knee replacement surgeons. We perform full spectrum of knee operations – from key-hole surgery (arthroscopy) to alignment correction (HTO), to capping (partial replacement) to knee replacement (TKR). We choose what is most suitable for our patient.
With our experience, we have been able to perfect the art of partial knee replacement, a real life-changing operation. The following are some of the highlights of our technique.
- We have been able to improve our success rate by the
following:
(a) Choosing the right patient: We have a strict protocol of choosing the patient. It includes getting a series of special knee x-rays done, some of which are hard to get done anywhere else. This helps us to evaluate whether only one part or more than one part of the knee are damaged – something very critical for the success of this operation. If still in doubt, we confirm the same by arthroscopy (looking inside the knee with a small camera) just prior to the operation. We are fully geared with all facilities in our OT, and take a call depending upon what will suit our patient. All this is possible as we are apt at all techniques of knee surgery –key-hole as well as open.
(b) The implant used: The implant (the artificial cap) we use is what is called 'mobile bearing'.This has three parts like any other partial knee but the middle plastic part is freely mobile and adjusts within the knee as per the forces inside the knee. It is popularly known as 'Oxford knee' as it was designed by a group of surgeons in Oxford, UK. This joint has the best track record, and is the most popular partial knee implant in the world. (c) The technique of fitting: We use the exacting technique of fitting the implant, using computer navigation wherever required. With this, we have been able to achieve perfect fixation and alignment even in obese patients.
(d) Optimize rest of the knee: When we do partial knee replacement, we do not leave it there. We also improve the rest of the knee, whatever way possible. This helps in prolonging the life of the knee.
- Pain control: We have a very regulated pain relief programme, and we want patient to have a painless pleasant experience of surgery
- No physiotherapy: Most of our patients do not need supervised physiotherapy after this operation. They do it themselves.
- Accessibility: Our team, including the senior surgeon is accessible on mobile phones to address all problems of the patients. We have a home care team to look after the patient's need if required.
- We do both knees together, if required.
This is what some of the patients have to Say...
“I used to have severe pain in both my knees – slept after taking Nise pill every night. I was advised to have total knee replacement on both my knees by other doctors…on the advise of Dr. Maheshwari, I underwent partial replacement…I felt I was given another life, no Nise , no pain – full 10 marks…People can't judge that I have had surgery on my knees unless I tell them – I am into my normal activities.”
Rekha Kanjilal (b.kanjilal@hotmail.com)
“I am feeling extraordinarily well aGer partial knee replacement. The satisfaction level i s totally unbelievable…The partial knee replacement has transformed my life…I do not have any problem at all. I can walk, sit with folded knee and am capable of performing all daily activitiesabsolutely normally and perfectly.”
Mr. Suresh Kumar Jindal (09958432121)
“I rate my experience of partial knee replacement as 10/10. Now 11 years aGer the surgery, I am 100% fit, and have no problem. I walk almost 4 KM every day.”
Mr. Rajiv Malaviya (9350836484)
...and many more similar experiences.
Our philosophy: Most important, we have a philosophy of treatment. We take every patient as a human being with different requirements – physical and psychological. We customize our treatment to patient's need. Our aim is to give our patient the experience of having gone through the treatment, what we would expect for our own relative. For us, by choosing us their doctor, the patient is giving us a great honour, and we value it. To showcase that we care, all our operated patients have direct access to cell phones of our team, including that of the chief surgeon.
MAP


